







.png)
The surgery had gone well.
After hours in the operating theatre at Great Ormond Street Hospital, the child’s heart had been repaired and the surgical team was beginning the final stage of the procedure. But in paediatric cardiac surgery, the end of an operation does not signal the end of risk.
Now came the handover.
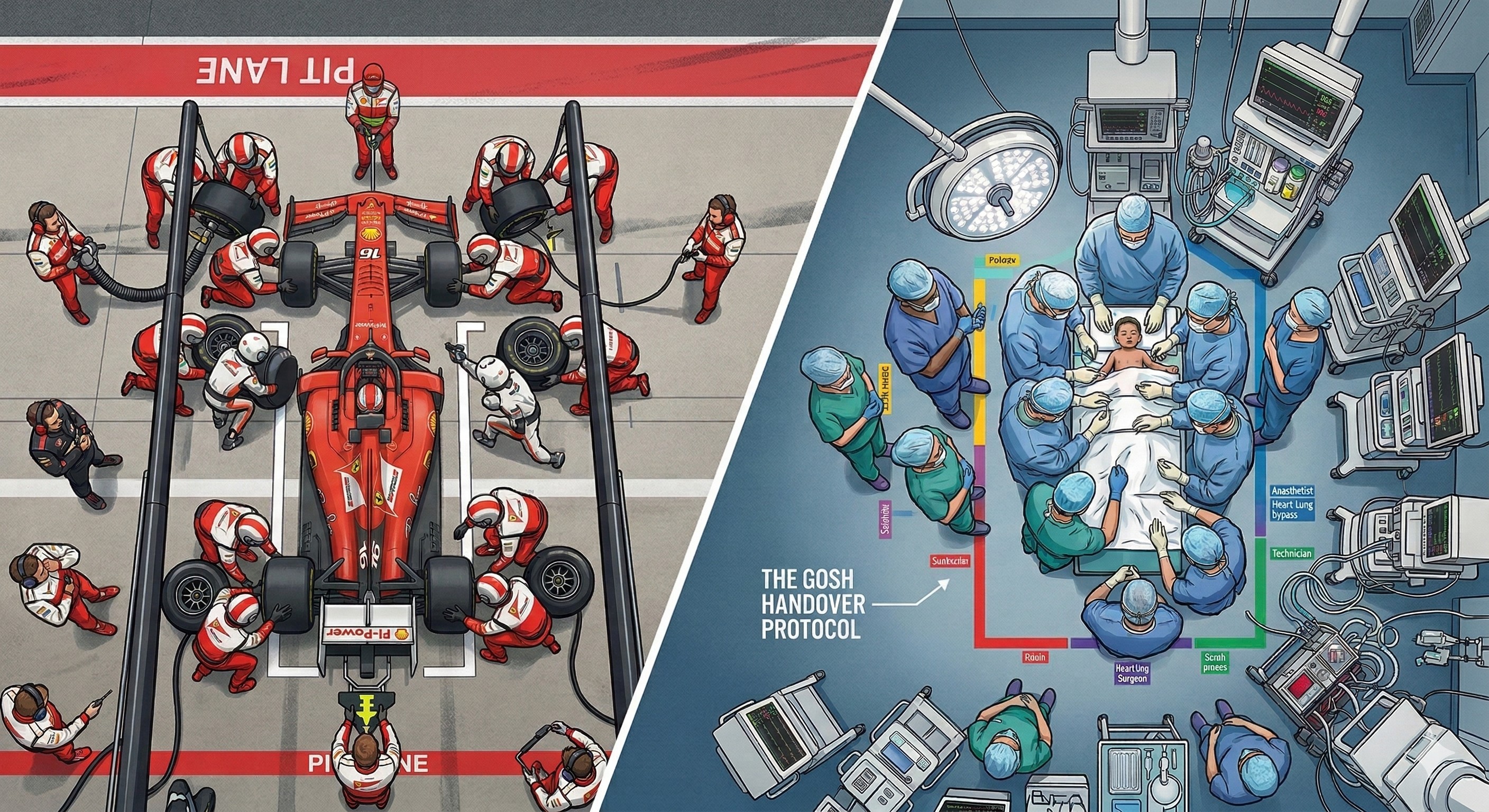
Ventilators, infusion pumps, monitoring lines and drainage tubes had to move with the patient as the team transferred the child from the operating theatre to intensive care. Around twenty clinicians and nurses crowded the room, each responsible for part of the process. Information needed to pass between teams at exactly the same moment equipment was being moved, lines reconnected and monitors re-established.
The journey itself was only a few corridors.
Yet within the hospital it had quietly developed a reputation as one of the most fragile moments in the entire surgical pathway. The process was complex, often noisy, and rarely performed exactly the same way twice. Even when surgery had gone perfectly, the transfer to intensive care could feel improvised — a swirl of conversations, movement and equipment in which small errors could easily occur.
For Martin Elliott, one of the hospital’s leading paediatric heart surgeons, that reality had become increasingly frustrating.
Later that day, between operations, Elliott and his intensive care colleague Dr Allan Goldman sat down briefly in the staff room. A Formula 1 race was playing on the television.
As Elliott watched, a car peeled into the pit lane.
Within seconds, more than twenty mechanics surrounded the vehicle. Tyres were removed. New ones were fitted. Adjustments were made. Moments later the car accelerated back onto the circuit.
What struck Elliott wasn’t the speed.
It was the choreography.
“I remember watching a Formula One pit stop and thinking, that’s exactly what we need to do when we move a child from the operating theatre to intensive care.”
— Professor Martin Elliott, Great Ormond Street Hospital
Because in paediatric cardiac surgery, the most fragile minutes are not always those spent repairing the heart.
Sometimes they begin when the operation ends.
When the Operation Ends — and the Risk Doesn’t
For children recovering from complex heart surgery, the transfer from the operating theatre to intensive care is deceptively demanding. The patient must move together with ventilators, infusion pumps, monitoring equipment and multiple clinical teams. At the same time, critical information about the operation must pass from the surgical team to intensive care clinicians. It is a moment where technical precision and communication must occur simultaneously.
Watching the pit stop unfold on television, Elliott recognised something familiar.
“A Formula One pit stop is a highly choreographed process involving many people doing different tasks in a very small space. The parallels with transferring a patient after surgery were obvious.”
— Professor Martin Elliott
Both environments involve highly specialised teams performing complex tasks under pressure. In Formula 1, that challenge had led to the meticulous design of pit-stop procedures — every movement rehearsed, every role defined.
Elliott wondered whether the same thinking could improve the reliability of surgical handovers.
Bringing Motorsport Thinking into Medicine
The idea sounded unconventional, but Elliott pursued it.
Clinicians at Great Ormond Street Hospital worked with a Formula 1 racing team to analyse and redesign the surgical handover process using pit-stop principles.
The engineers approached the operating theatre the same way they would study the pit lane.
They observed how clinicians moved around the patient.
They mapped the flow of equipment.
They studied how information was communicated during the transfer.
What they saw was familiar — because Formula 1 pit stops once looked similar before teams began systematically redesigning them.
“We weren’t looking at the medicine. We were looking at the process — how people moved, how they communicated, and where the opportunities for error existed.”
— Formula One engineering team member involved in the collaboration
The engineers were not evaluating surgical skill.
They were evaluating the system in which that skill was being applied.
Turning a Patient Transfer into a Pit Stop
Working together, clinicians and engineers redesigned the transfer from theatre to intensive care.
Each member of the team was given a clearly defined role, eliminating duplication and uncertainty.
The sequence of events became choreographed: who moved first, who positioned equipment, and when key information was communicated.
Equipment placement was standardised, ensuring clinicians did not have to reorient themselves during every transfer.
Communication was simplified into structured verbal cues, reducing the risk of overlapping conversations or missed information.
And perhaps most importantly, the team began rehearsing the transfer process — something routine in motorsport but uncommon in healthcare at the time.
The objective was not simply speed.
It was reliability.
What Changed — Measurably
The redesigned process was evaluated in a study published in BMJ Quality & Safety.
The results were significant.
Technical errors during patient handovers fell from 5.42 to 3.15 per transfer — a reduction of roughly 42 percent. Information omissions during handover dropped from 2.09 to 1.07, almost halving communication failures.
The average duration of the transfer also improved modestly, decreasing from 10.8 minutes to 9.4 minutes. Perhaps most strikingly, the proportion of patients experiencing multiple technical and communication failures fell from 39 percent to 11.5 percent.
“After introducing the pit-stop style handover, technical errors during patient transfer fell by more than forty percent.”
— Findings reported in BMJ Quality & Safety
These errors were not trivial details. They included temporary disconnections of monitoring equipment, delays reconnecting critical devices, or confusion during the clinical briefing that accompanies the transfer.
Reducing them makes the most vulnerable patients safer.
Mortality itself was not the primary metric — paediatric cardiac surgery already has relatively low mortality rates in leading centres — but reducing the conditions that allow harm to occur is one of the most effective ways to improve patient safety.
The Insight That Stayed with Surgeons
What fascinated many clinicians about the collaboration was not that Formula 1 made hospitals faster.
It was that the engineers approached the problem differently.
They did not focus on the expertise of individual clinicians.
They focused on how the system supported the team.
“Healthcare tends to focus on the performance of individuals. What Formula One understands is the performance of the team.”
— Professor Martin Elliott
In Formula 1, success depends on the choreography of the entire crew.
The same principle applies in medicine.
A Lesson Beyond the Racetrack
At first glance, Formula 1 racing and paediatric surgery seem worlds apart.
One unfolds on a racetrack at extraordinary speed, surrounded by noise and spectacle. The other takes place in the quiet intensity of an operating theatre, where the stakes are measured in human lives.
Yet both demand exceptional levels of precision, teamwork and trust.
The connection between them did not emerge from a strategy meeting or a research laboratory.
It began with a tired surgeon watching a pit stop between two operations — and recognising that excellence in one world might help save lives in another.
As engines roar again at the Australian Grand Prix during Melbourne’s 2026 Formula 1 week, millions of fans will marvel at teams shaving fractions of a second from a tyre change.
Few will realise that the same thinking — the choreography of high-performance teamwork — has already travelled far beyond the racetrack, quietly improving the safety of children recovering from heart surgery.
Researched and Written By: Bernard Herrok, proofed by AI.
Our Partners
.png)





Contact us



